
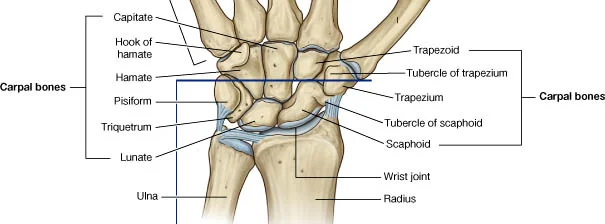
The carpal bones are a group of eight small bones in your hand. These include
Scaphoid (Most common 40-70% in literature)
Lunate (0/5% - 1% rare due to protected position in proximal carpal row)
Capitate (rare due to its protect position in the middle of the carpus)
Trapezium (4-5% of fractures)
Trapezoid (0.5-1%)
Triquetrum (2nd most common 4-18% in literature)
Hamate (2% of all fractures (Hook of hamate often a golf club versus ground)
Pisiform (<1% off all carpal fractures)
Scaphoid Fractures
The most common type of carpal bone fracture is a scaphoid fracture most likely because it is the easiest to identify on a plain x-ray in comparison to other bones. Having said that it can often not seen (known as an occult fracture) then an MRI or CT scan is recommended. Due to the blood supply which passes the bone and has a branch that reverts back the bone is at risk of death (avascular necrosis) or non union (not healing) therefore it is pertinent not to miss this injury.
Treatment in the acute stages is often splinting and review x-ray in 2 weeks is suspicious of a scaphoid fracture. Hand physiotherapist can make a splint to immobilise the wrist and this often includes the thumb. Once confirmed immobilisation can be from 6-12 weeks. With a injury like this it is recommended to work with your physio and sports physician (Sports doctor) to best guide the appropriate treatment pathway if conservative management is not appropriate.
Hulsopple et al (2017) Treatment of acute carpal bone fractures. Current Sports Medicine Reports